Histology
Biomimetic tissue architecture
The decisive role of circular fibers in protecting the biological width.
- Patented zirconia collar
- Titanium body
- Clinical versatility
- Protective barrier
- Tissue stability
- 98.8% Paro-Integration
- Aesthetics
- EU-MDR
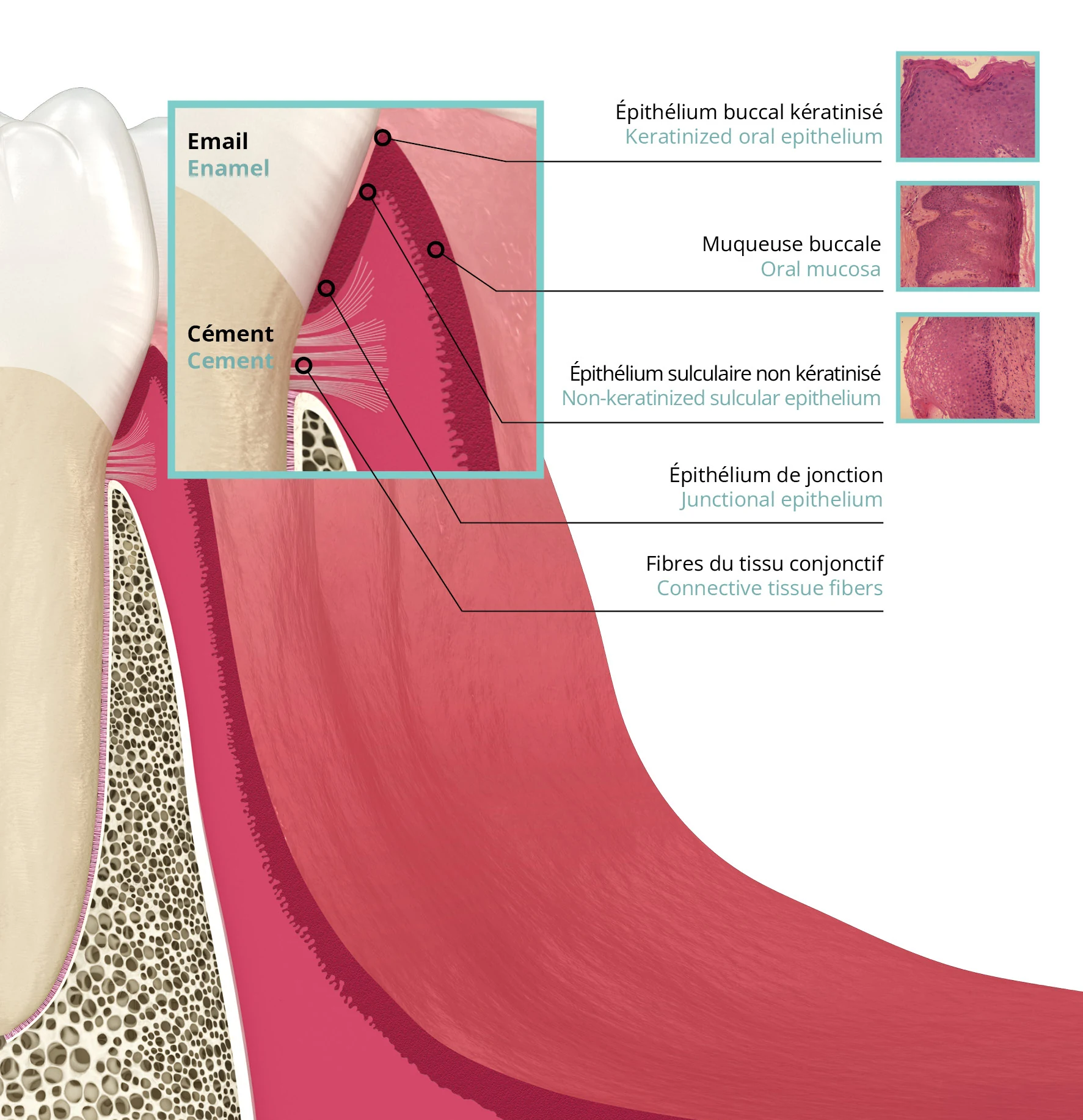
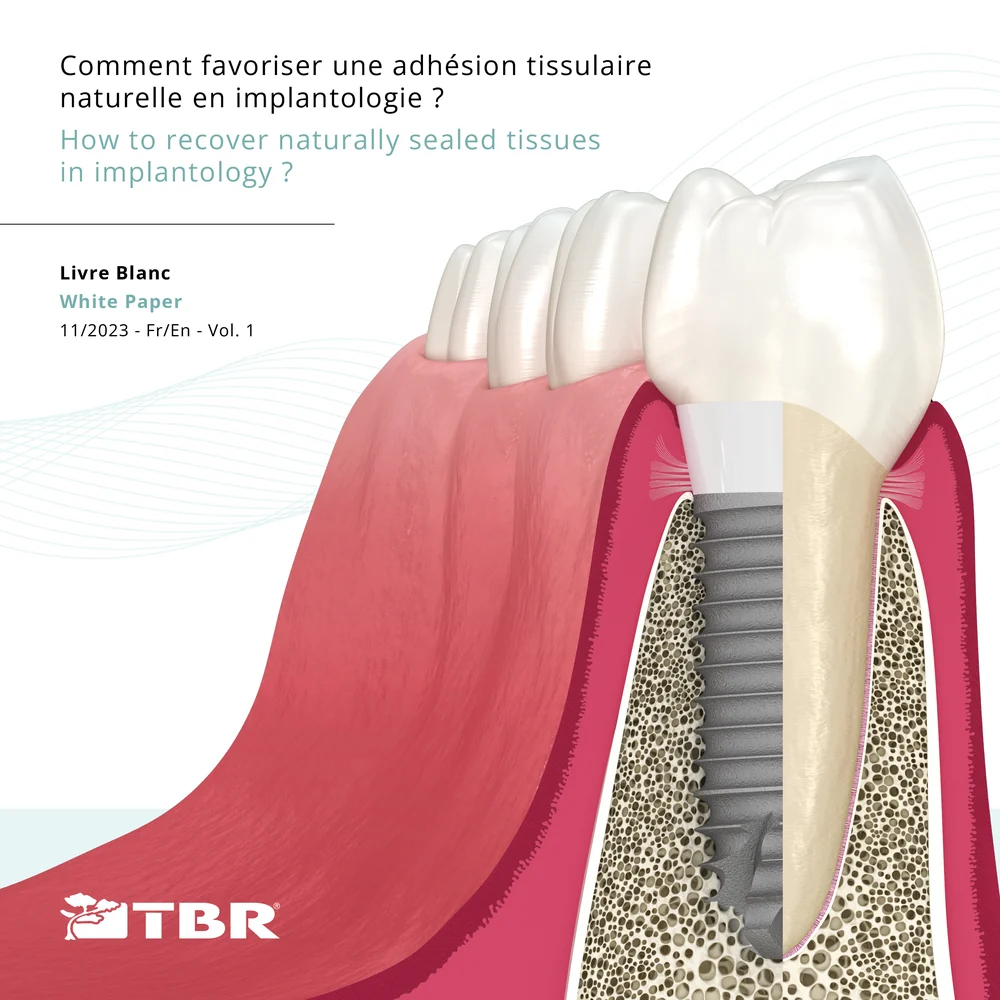
Balance of the epithelial-connective tissues around the natural tooth
Around a natural tooth, tissue integrity and stability are guaranteed by:
- At the epithelial level = a keratinised oral mucosa, a keratinised oral epithelium at the top of the sulcus, a non-keratinised sulcular epithelium followed by a short junctional epithelium in contact with the enamel. The presence of hemidesmosomes ensures the adhesion of this epithelium to the enamel of the tooth.
- At the connective level = a sleeve composed of a dense network of collagen fibers that adhere to the cementum.
The primary function of this complex architecture is to seal hermetically the supracrestal zone in order to protect and preserve the bone tissue from inflammatory and infectious threats originating from the oral cavity.
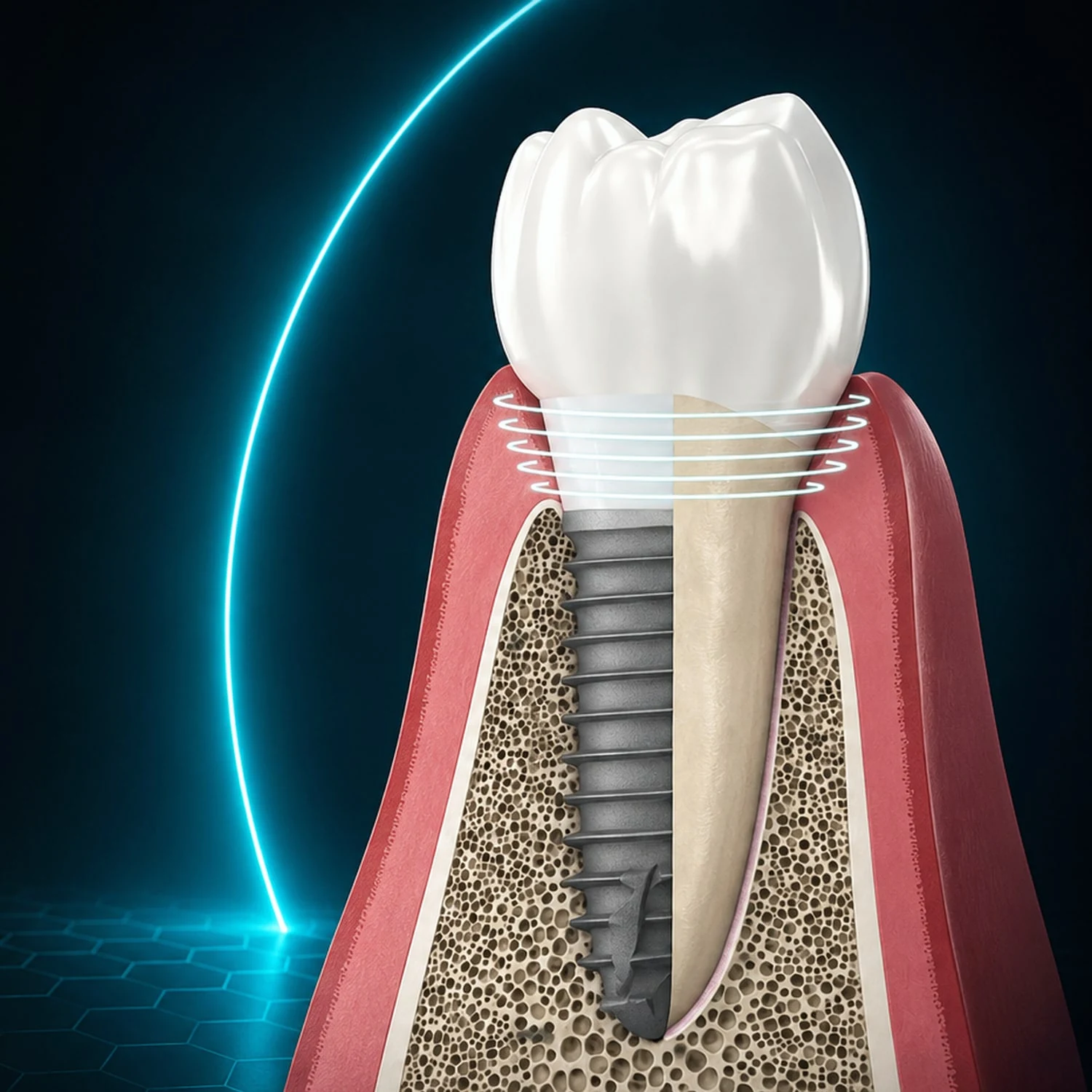
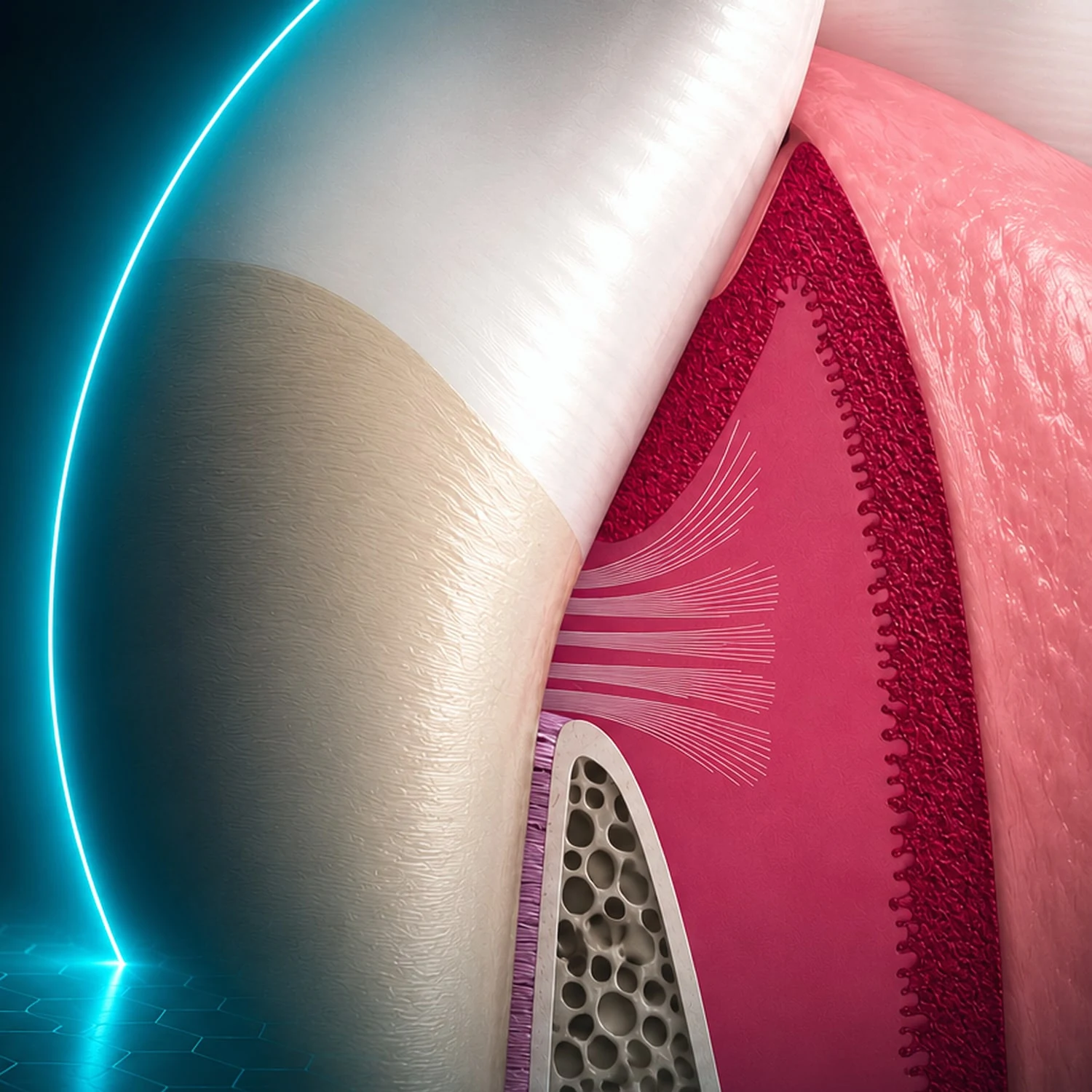
Focus on the biological width
This critical zone extends from the deepest point of the sulcus to the crestal bone. A dense network of oblique and circular fibers straps and supports these anatomical soft tissues.
Comparison of the cervical attachment system between a tooth and an implant
At the supracrestal level, the oblique fibers, anchored perpendicularly into the cement, provide a true biological attachment by preserving the periodontal health.
The mechanical action of the circular fibers seals and protects the underlying periodontal tissues.
-
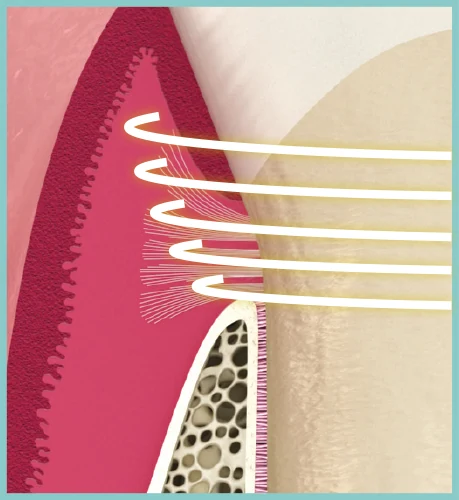
Behaviour of connective fibers in contact with a tooth
The combination of oblique and circular fibers acts to seal the cervical contour, maintains a functional volume of connective tissue and, most importantly, prevents epithelial invagination.
The short junctional epithelium thus formed is maintained at a healthy distance from the bone crest.
-
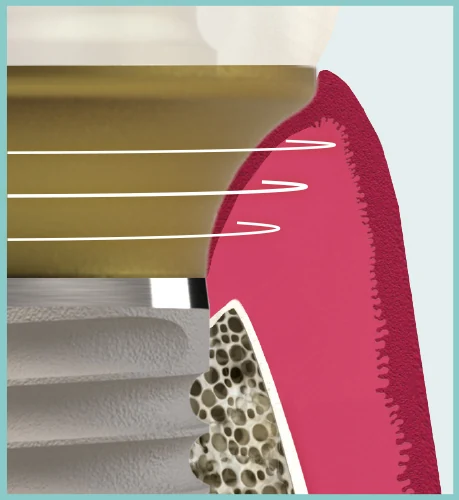
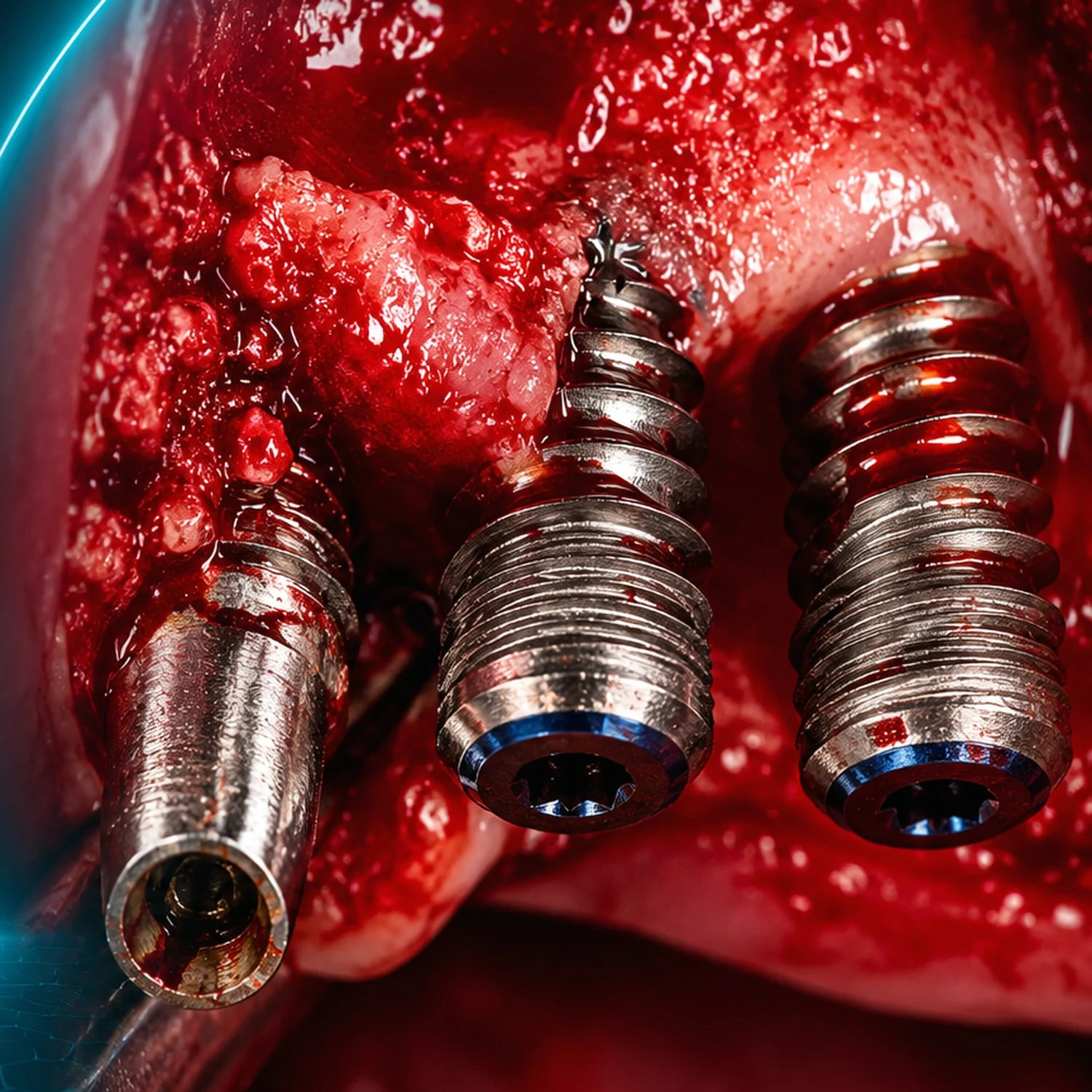
Behaviour of connective fibers in contact with an implant
The biological width surrounding an implant results from a physical adaptation rather than an actual biological attachment.
The collagen fibers are not anchored to either the implant or the prosthetic component, and are oriented randomly. Fewer circular fibers are embedded in a less dense connective tissue.
A descending invagination of the junctional epithelium is observed following implant placement. This long junctional epithelium does not form an anchor around the implant or prosthetic surface.